 PDF(1650 KB)
PDF(1650 KB)

计算机辅助认知康复训练对脑卒中患者总体认知功能改善的Meta分析
公冶慧娟, 徐潇潇, 王皎, 刘沙沙
PDF(1650 KB)
计算机辅助认知康复训练对脑卒中患者总体认知功能改善的Meta分析
Computer aided cognitive rehabilitation training on overall cognitive function improvement in stroke patients: a meta-analysis
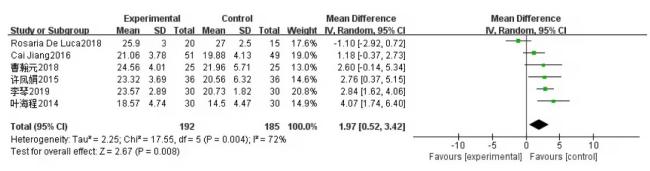
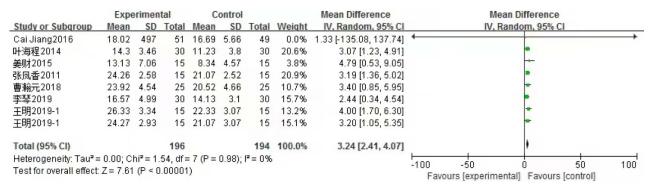
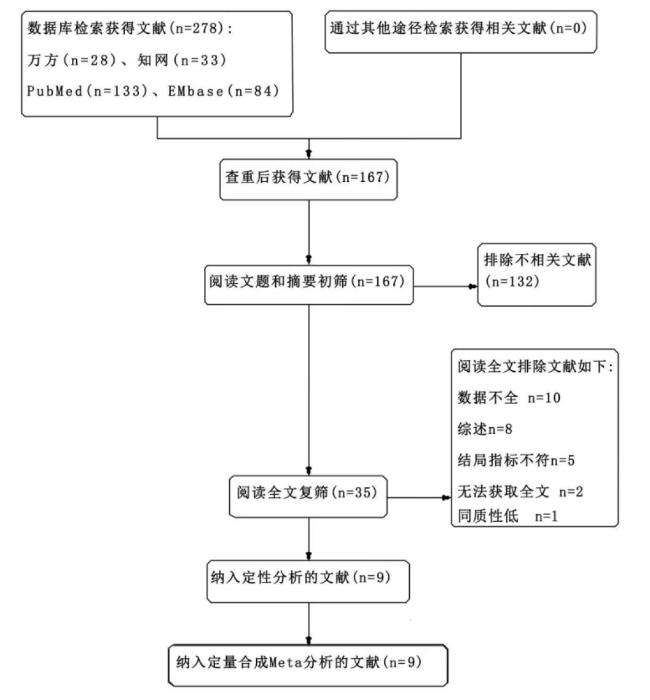
目的: 评价计算机辅助认知康复训练对脑卒中后认知损害患者总体认知功能的改善效果。方法: 计算机检索Pubmed、EMbase、万方和CNKI数据库,搜集关于计算机辅助认知康复训练对脑卒中后认知损害患者总体认知功能改善效果的随机对照研究,时限为建库到2022年5月。文献的筛选、资料的提取和评价纳入研究的偏倚风险由2名研究者独立完成,最后采用RevMan5.3软件进行Meta分析。结果: 共纳入9个RCT研究,包括467例患者。Meta分析结果显示,MMSE的效应值是1.97 [0.52, 3.42],MoCA的效应值是3.24[2.41,4.07]。在认知功能改善方面,计算机辅助认知康复训练效果优于人工认知康复训练。结论: 4周及以上计算机辅助认知康复训练在改善脑卒中患者总体认知功能方面存在优势,临床上可根据不同患者、不同医院的具体情况制定康复方案,使认知功能得到有效的改善。受纳入研究数量和质量的限制,结论尚待更多高质量研究予以验证。
Objective: To systematically evaluate the effect of computer aided cognitive rehabilitation training on the overall cognitive function of patients with cognitive impairment after stroke. Methods: Pubmed, EMbase, Wanfang and CNKI databases were searched by computer to collect randomized controlled trials on the effect of computer aided cognitive rehabilitation training on the improvement of overall cognitive function in patients with cognitive impairment after stroke. The time limit was from the establishment of the database to May 2022. Literature screening, data extraction and bias risk assessment of included studies were completed by two researchers independently. Finally, RevMan5.3 software was used for Meta-analysis. Results: Nine RCTs involving 467 patients were included. Meta-analysis results showed that the effect size of MMSE was 1.97 [0.52, 3.42]. Meta-analysis results showed that the effect size of MoCA was 3.24[2.41, 4.07].In terms of cognitive function improvement, computer aided cognitive rehabilitation training is better than artificial cognitive rehabilitation training. Conclusion: Computer aided cognitive rehabilitation training for more than 4 weeks has advantages in improving the cognitive function of stroke patients. Rehabilitation programs can be made according to the specific conditions of different patients and different hospitals, so as to improve the cognitive function effectively. Limited by the quantity and quality of the included studies, the conclusions need to be verified by more high-quality studies.
计算机辅助认知康复 / 脑卒中 / 总体认知功能 / Meta分析 {{custom_keyword}} /
Computer aided cognitive rehabilitation / Stroke / Global cognitive function / Meta analysis {{custom_keyword}} /
表1 纳入研究的基本特征Tab 1 Basic features of included studies |
| 纳入研究 | 国家 | 样本量(人) 干预组/对照组 | 平均年龄(岁) 干预组/对照组 | 干预措施 | 结局指标 | 干预时间 | 具体值(x±s) |
|---|---|---|---|---|---|---|---|
| 李琴[7]2019 | 中国 | 30/30 | 64.67/66.57 | 常规康复治疗+计算机认知康复/常规康复治疗 | MMSE和MoCA得分 | 4周 | 20.73±1. 82 23.57±2. 89 14.13±3. 10 16.57±4. 99 |
| 王明[8]2019 | 中国 | 15/15 | 未提及 | 常规康复治疗+计算机辅助认知训练/常规康复治疗 | MoCA得分 | 8周 | 21.07±3.07 24.27±2.93 22.33±3.07 26.33±3.34 |
| 曹瀚元[9]2018 | 中国 | 25/25 | 57.12/56.96 | 常规康复治疗+计算机辅助康复治疗/常规康复治疗 | MMSE和MoCA得分 | 8周 | 21.96±5.71 24.56±4.01 20.52±4.66 23.92±4.54 |
| 姜财[10]2015 | 中国 | 15/15 | 63.90/62.2 | 常规康复治疗+计算机辅助认知训练/常规康复治疗 | MoCA得分 | 12周 | 8.34±4.57 13.13±7.06 |
| 许凤娟[11]2015 | 中国 | 36/36 | 60.65/56.71 | 常规康复治疗+计算机辅助认知障碍训练/常规康复治疗+人工认知训练 | MMSE得分 | 8周 | 20.56±6.32 23.32±3.69 |
| 叶海程[12]2014 | 中国 | 30/30 | 60.33/60.33 | 常规康复治疗+计算机辅助认知训练/常规康复训练 | MMSE和MoCA得分 | 8周 | 14.50±4.47 18.57±4.74 11.23±3.80 14.30±3.46 |
| 张凤香[13]2011 | 中国 | 15/15 | 65.95/64.59 | 常规康复训练+计算机认知康复训练/常规康复训练 | MoCA得分 | 8周 | 21.07±2.52 24.26±2.58 |
| Rosaria De Luca[14]2018 | 意大利 | 20/15 | 43.90/ 42.10 | 计算机认知康复/传统康复训练 | MMSE得分 | 8周 | 22.70±2.50 27.00±2.50 23.80±3.50 25.90±3.00 |
| Cai Jiang[15]2016 | 中国 | 51/49 | 63.90/62.20 | 常规康复治疗+计算机辅助认知康复/常规康复治疗 | MMSE和MoCA得分 | 12周 | 19.88±4.13 21.06±3.78 16.69±5.66 18.02±4.97 |
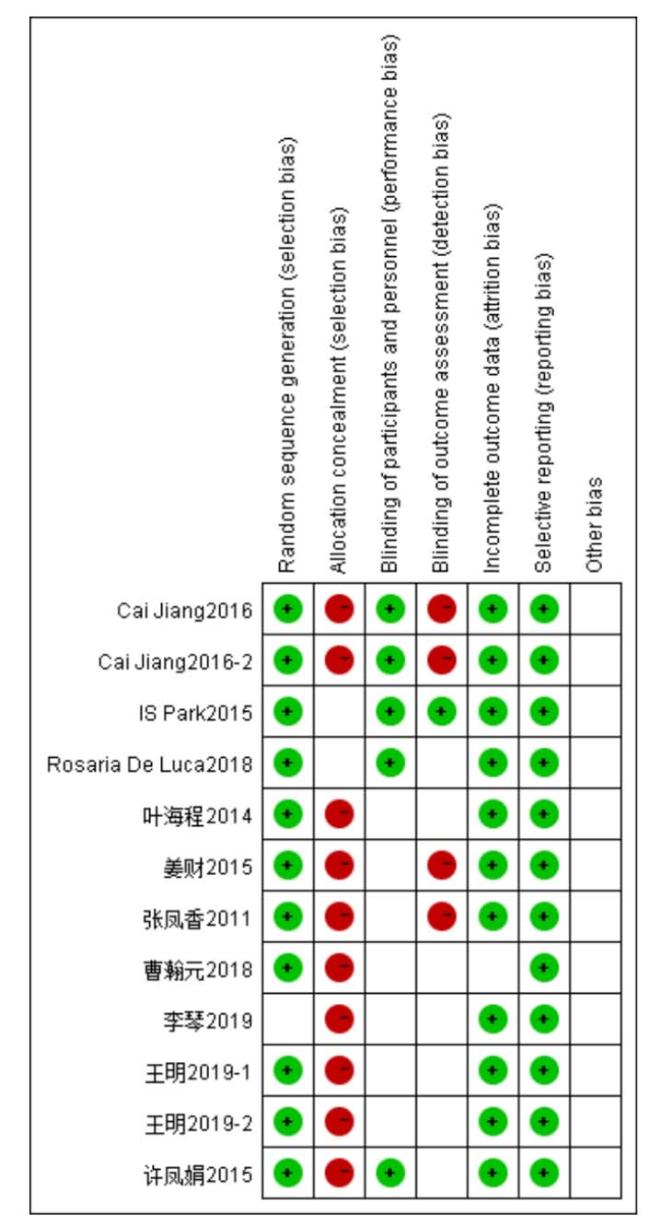
| 注:使用2014版Cochrane偏倚风险评估工具对纳入的RCT研究进行评估 | |
| Note:The Cochrane Risk of Bias tool (version 2014) was used to evaluate the included RCT studies |
| [1] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [2] |
Few studies exist on subjective cognitive failures after a stroke in young adults (≤50 years) and their relation to objective cognitive performance is unknown. Therefore, we investigated the prevalence of subjective cognitive failures in patients with a stroke in young adulthood and their relation with objective cognitive impairment. This study is part of the "Follow-Up of Transient ischemic attack and stroke patients and Unelucidated Risk factor Evaluation"-study (FUTURE study), including patients, aged 18-50 years, admitted to our hospital between 1980 and 2010 with a first-ever TIA or ischemic stroke. The prevalence of subjective cognitive failures in patients was determined and compared with 146 age- and sex-matched stroke-free controls. The relation of subjective failures with objective cognitive performance was investigated with linear and logistic regression analysis. 160 patients with a TIA and 277 with an ischemic stroke were included. After a mean follow-up of 10.1 (SD 8.3) years, the prevalence of subjective memory failures was 86.4% and that of subjective executive failures was 67.4% in patients, versus 69.7% (p = 0.008) and 41.4% (p = 0.002) in controls. A weak association between subjective memory failures and objective immediate (beta -0.12, p = 0.011) and delayed memory performance (beta -0.13, p = 0.010) was observed in patients. Subjective cognitive failures are prevalent after stroke in young adults, but not strongly related to objective cognitive impairment. Therefore, extensive neuropsychological assessment is essential for determination of objective cognitive impairment. However, it is important that subjective cognitive failures are recognized as they may indicate underlying psychosocial problems.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [3] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [4] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [5] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [6] |
Cognitive impairment after stroke has a direct impact on daily functioning and quality of life (QoL) of patients and is associated with higher mortality and healthcare costs. The aim of this study was to determine the effect of a computer-based brain training programme on cognitive functioning, QoL and self-efficacy compared to a control condition in stroke patients. Stroke patients with self-perceived cognitive impairment were randomly allocated to the intervention or control group. The intervention consisted of an 8-week brain training programme (Lumosity Inc.®). The control group received general information about the brain weekly. Assessments consisted of a set of neuropsychological tests and questionnaires. In addition, adherence with trained computer tasks was recorded. No effect of the training was found on cognitive functioning, QoL or self-efficacy when compared to the control condition, except for very limited effects on working memory and speed. This study found very limited effects on neuropsychological tests that were closely related to trained computer tasks, but no transfers to other tests or self-perceived cognitive failures, QoL or self-efficacy. These findings warrant the need for further research into the value of computer-based brain training to improve cognitive functioning in the chronic phase after stroke.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [7] |
李琴, 陈嘉卿, 李雨峰, 等. 计算机辅助康复治疗对脑卒中后认知功能障碍的影响[J]. 实用医院临床杂志, 2019, 016(2):188-190.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [8] |
王明. 计算机辅助认知康复结合小组认知训练对脑卒中患者认知功能的疗效[J]. 微循环学杂志, 2019, 029(1):43-47
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [9] |
曹瀚元, 夏文广, 郑婵娟, 等. 计算机辅助认知训练对脑卒中后不同程度认知障碍康复疗效的影响[J]. 生物医学工程与临床, 2018, 22(6):633-637.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [10] |
姜财, 杨珊莉, 黄佳, 等. 计算机辅助认知训练对脑卒中患者认知功能恢复的影响及其机制的fMRI研究[J]. 中国康复医学杂志, 2015, 30(9):911-914.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [11] |
许凤娟, 黄丽虹, 倪朝民, 等. 计算机辅助认知训练对脑卒中患者认知功能的影响[J]. 安徽医药, 2015, 000(8):1519-1520.
[ 12 叶海程, 杨珊莉, 陈立典, 等. 计算机辅助认知训练对脑卒中患者认知功能及功能独立性的影响[J]. 实用医学杂志, 2014, 000(17):2742-2744.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [13] |
张凤香, 邢昂, 郭宗君, 等. 计算机认知训练对脑卒中后认知功能障碍康复的影响[J]. 医学信息, 2011, 24(6):3378-3379.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [14] |
Cognitive impairment after stroke is common and can cause disability with a high impact on quality of life and independence. Cognitive rehabilitation is a therapeutic approach designed to improve cognitive functioning after central nervous system's injuries. Computerized cognitive rehabilitation (CCR) uses multimedia and informatics resources to optimize cognitive compromised performances. The aim of this study is to evaluate the effects of pc cognitive training with Erica software in patients with stroke.We studied 35 subjects (randomly divided into 2 groups), affected by either ischemic or hemorrhagic stroke, having attended from January 2013 to May 2015 the Laboratory of Robotic and Cognitive Rehabilitation of Istituto di Ricerca e Cura a Carattere Scientifico Neurolesi in Messina. Cognitive dysfunctions were investigated through a complete neuropsychological battery, administered before (T0) and after (T1) each different training.At T0, all the patients showed language and cognitive deficits, especially in attention process and memory abilities, with mood alterations. After the rehabilitation program (T1), we noted a global cognitive improvement in both groups, but a more significant increase in the scores of the different clinical scales we administered was found after CCR.Our data suggest that cognitive pc training by using the Erica software may be a useful methodology to increase the post-stroke cognitive recovery.Copyright © 2018 National Stroke Association. Published by Elsevier Inc. All rights reserved.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [15] |
The aim of this study was to identify the clinical efficacy of acupuncture in combination with RehaCom cognitive training in poststroke patients with cognitive dysfunction.This study was a 2 × 2 factorial design randomized controlled trial comparing acupuncture, computer-assisted cognitive rehabilitation, and the usual treatment by per-protocol analysis. The trial was completed by 204 stroke patients, including 49 patients in a control group, 52 patients in an acupuncture treatment group, 51 patients in a RehaCom training group, and 52 patients in an acupuncture combined with RehaCom group. All of the patients accepted basic treatment and health education. The interventions continued for 12 weeks (30 minutes per day, 5 days per week). The relative cognitive and functional outcomes were measured at baseline and 12 weeks (at the end of intervention) using the Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), and Functional Independence Measure (FIM) scales.After 12 weeks of treatment, the functional statuses of the patients in each of the 4 groups showed varying degrees of improvement. Multiple comparisons of the changes in the MMSE, MoCA, and FIM scores indicated that acupuncture combined with RehaCom cognitive training (ACR) had enhanced therapeutic effects on the functional statuses of the stroke patients (P < .05). In addition, ACR had similar therapeutic effects on the functional statuses of the stroke patients according to each of the assessment scales applied (P△ MMSE = 0.399, P△MoCA = 0.794, P△FIM = 0.862). The interaction effect values between acupuncture and RehaCom training (acceptance or nonacceptance) were as follows: △MMSE: F = 6.251, P = .013; △MoCA: F = 4.991, P = .027; and △FIM: F = 6.317, P = .013. Further, the main effect values for acupuncture and RehaCom training were both significant (P < .05).There is an interaction effect in the treatment of stroke patients using ACR. The use of acupuncture in combination with RehaCom training has better therapeutic effects on the functional statuses of poststroke patients than the use of either treatment alone, demonstrating the clinical significance of this combination therapy.Copyright © 2016 AMDA – The Society for Post-Acute and Long-Term Care Medicine. Published by Elsevier Inc. All rights reserved.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [16] |
国家统计局, 中华人民共和国2022年国民经济和社会发展统计公报[R/OL][2022-04-15]. https://www.stats.gov.cn/zt_18555/zthd/lhfw/2023/hgjj/202302/t20230228_1919008.html
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| {{custom_ref.label}} |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
PDF(1650 KB)
 表1 纳入研究的基本特征
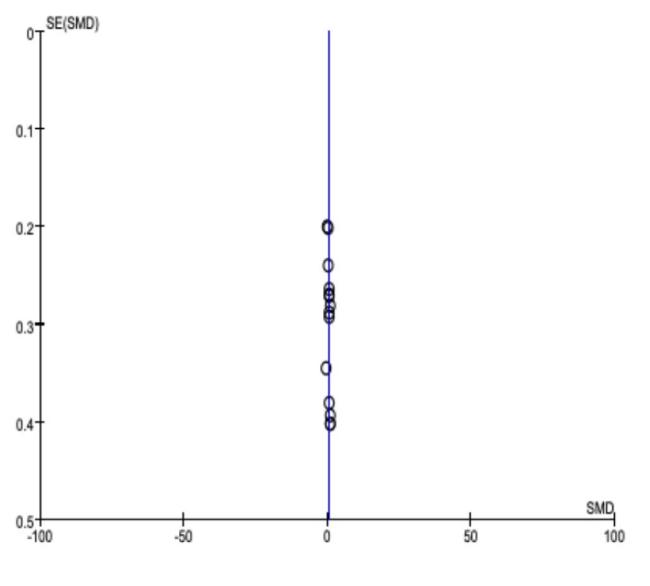
表1 纳入研究的基本特征 图2 纳入研究的偏倚风险评价结果图3 MMSE评分比较的Meta分析结果图4 MoCA评分比较的Meta分析结果图5 偏倚性分析图1 文献筛选流程
图2 纳入研究的偏倚风险评价结果图3 MMSE评分比较的Meta分析结果图4 MoCA评分比较的Meta分析结果图5 偏倚性分析图1 文献筛选流程/
| 〈 |
|
〉 |


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}