 PDF(804 KB)
PDF(804 KB)

Correlations between cognitive reserve and gray matter volume and cognitive impairment in patients of Alzheimer’s disease
GAO Ziwen, ZHU Wanqiu, LI Xiaoshu, LI Meiqin, ZHOU Shanshan, TIAN Yanghua, WU Xingqi, GENG Zhi, LI Xiaohu, YU Yongqiang
PDF(804 KB)
Correlations between cognitive reserve and gray matter volume and cognitive impairment in patients of Alzheimer’s disease
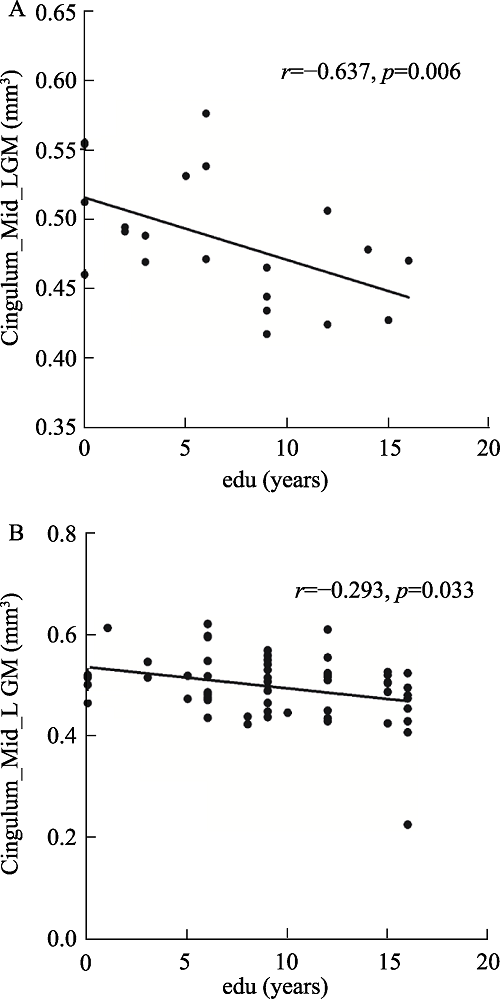
Objective: Education can be used to reflect cognitive reserve (CR), in this study, we aimed to explore the relationship between education level and changes of brain gray matter volume (GMV) as well as the progression of cognitive impairment in Alzheimer’s disease (AD) patients. Methods: Fifty-seven patients with AD (further divided into mild, moderate and sever groups according to the severity of dementia), 57 patients with amnestic mild cognitive impairment (aMCI) and 52 healthy controls (HC) were collected in this study to obtain high-resolution 3-dimensional T1 structure images. GMV of brain regions related to educational years in AD patients were obtained using VBM8 and SPM8 software, which were then taken as the regions of interest (ROI). The correlation analyses between GMV of ROIs and education were conducted in HC, aMCI, mild, moderate, and severe AD group, separately. AD and aMCI patients were divided into high cognitive reserve (CR+) group and low cognitive reserve (CR-) group according to the median years of education within the entire cognitive impairment sample. The GMV of ROIs were compared in CR+ and CR-groups at each cognitive level. Results: In AD group, the GMV of the left middle cingulate cortex was negatively correlated with the years of education (FDR correction, P< 0.05). Further stratified analysis showed that it was only negatively correlated with the years of education in mild AD group and aMCI group (r=-0.637, P= 0.006 and r =-0.293, P=0.033, respectively). In addition, in mild and moderate AD groups, the GMV of left middle cingulate cortex in CR+ group was significantly lower than that in CR- group (both P< 0.05). Conclusion: AD patients with higher education showed more severe gray matter volume atrophy of the left middle cingulate cortex at a given level of global cognition, reflecting the notion that AD patients with higher reserve can withstand a greater amount of pathology, which confirms the protection effect of cognitive reserve on AD patients.
Alzheimer’s Disease / Amnestic mild cognitive impairment / Cognitive reserve / Magnetic resonance imaging / Voxel-based morphometry {{custom_keyword}} /
表1 基本人口学资料 |
| 指标 | HC (n=52) | aMCI (n=57) | AD(n=57) | P值 |
|---|---|---|---|---|
| 年龄/岁 | 66.38±7.3 | 66.33±7.47 | 67.74±8.28 | 0.55 |
| 性别(男/女) | 20/32 | 26/31 | 22/35 | 0.678 |
| 教育程度/年 | 11.65±3.42 | 9.37±4.77 | 6.14±5.38 | <0.001* |
| MMSE | 28.58±1.18 | 26.35±1.58 | 15.28±5.22 | <0.001* |
| 颅内总体积/mm3 | 1 371.12±102.691 | 1 352.925±99.695 | 1 314.274±109.086 | 0.015* |
| 注:连续变量组间比较采用单因素ANOVA;分类变量组间比较采用卡方检验。*P< 0.05,说明差异有统计学意义。 |
表2 左中扣带灰质体积值分组与教育程度的相关性 |
| 分组 | HC (n=52) | aMCI (n=57) | 轻度AD (n=21) | 中度AD (n=22) | 重度AD (n=14) |
|---|---|---|---|---|---|
| 左中扣带回体积与教育程度的相关性 | r=-0.065 P=0.659 | r=-0.293* P=0.033 | r=-0.637* P=0.006 | r=-0.296 P=0.233 | r=-0.411 P=0.239 |
| 注:*P< 0.05,说明差异有统计学意义。 |

图1 AD患者脑灰质体积与教育程度的相关性注:a~c显示与教育相关的脑区(左侧中扣带回),FDR校正,P< 0.05; d为左侧中扣带回灰质体积与教育年限相关性分析的散点图。 |
表3 相同认知水平下CR+和CR-组的组间比较 |
| aMCI(n=57) | 轻度AD(n=21) | 中度AD(n=22) | 重度AD(n=14) | |||||
|---|---|---|---|---|---|---|---|---|
| CR-(n=22) | CR+(n=35) | CR-(n=12) | CR+(n=9) | CR-(n=15) | CR+(n=7) | CR-(n=7) | CR+(n=7) | |
| 年龄/年 | 64.79±6.57 | 68.46±8.22 | 66.58±5.66 | 70.22±7.68 | 69.27±7.36 | 62.86±9.33 | 63.71±7.34 | 72.14±12.13 |
| 性别(男/女) | 9/13 | 17/18 | 6/6 | 3/6 | 5/10 | 3/4 | 2/5 | 3/4 |
| MMSE | 26.18±1.65 | 26.58±1.47 | 19.83±3.19 | 20.67±2.12 | †*12(11-14) | 17.43±1.72* | 7.86±5.11 | 10.86±1.46 |
| 颅内总体积/mm3 | 1353.17± 97.12 | 1352.59± 105.25 | 1341.59± 95.19 | 1314.34± 112.45 | 1312.50± 98.90 | 1290.83± 123.87 | 1322.10± 123.65 | 1286.79± 145.08 |
| 左扣带回灰质体积/mm3 | 0.51±0.05 | 0.48±0.06 | 0.51±0.04* | 0.45±0.03* | 0.50±0.04* | 0.44±0.05* | 0.44±0.05 | 0.431±0.04 |
| 注:符合正态分布连续变量数据采用独立双样本t检验,†表示数据不满足正态分布,采用非参数秩和检验;分类变量采用卡方检验及Fisher精确检验。*P< 0.05,差异具有统计学意义。将aMCI与AD纳入认知损害组,并根据痴呆严重程度将AD分为轻、中、重组。依据教育年限中位数将患者分为高认知储备(CR+)组与低认知储备(CR-)组。在MCI、轻、中、重AD各组内,CR+分别与同组内的CR-相比较。 |
| [1] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [2] |
杨宁, 徐盼盼, 刘佩嘉, 等. 基于张量法的阿尔兹海默症脑图像分类[J]. 中山大学学报(自然科学版), 2017, 56(2): 40-47.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [3] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [4] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [5] |
林岚, 张柏雯, 王婧璇, 等. 认知储备在大脑老化中的研究进展[J]. 医疗卫生装备, 2017, 38(9): 93-98.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [6] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [7] |
Cognitive reserve theory helps to explain the neuropsychological expression of neurologic disease (e.g., Alzheimer's disease; Stern, 2006). Multiple sclerosis (MS) is a neurologic disease characterized by information processing inefficiency and verbal learning and memory deficits. The current study is the first to investigate whether higher cognitive reserve moderates the relationship between MS and cognitive functioning. A word-reading proxy of premorbid intelligence was used to estimate cognitive reserve for 58 persons with MS and 43 healthy controls. Dependent measures of simple processing efficiency, complex information processing efficiency, and verbal learning and memory were administered. There were significant Group x Cognitive Reserve interactions for complex information processing efficiency and verbal learning and memory, such that persons with MS demonstrated deficits relative to controls at lower, but not higher, levels of reserve. No such interaction was found for simple processing efficiency. The protective influence of higher cognitive reserve against disease-related cognitive deficits is discussed.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [8] |
Postmortem examination was performed on 137 residents (average age 85.5 years) of a skilled nursing facility whose mental status, memory, and functional status had been evaluated during life. Seventy-eight percent were demented using conservative criteria; 55% had characteristic Alzheimer's disease. Choline acetyltransferase and somatostatin were significantly reduced in the brains of patients with Alzheimer's disease as compared with age-matched nursing home control subjects, although the degree of the reduction was less severe than found in subjects less than 80 years of age. Ten subjects whose functional and cognitive performance was in the upper quintile of the nursing home residents, as good as or better than the performance of the upper quintile of residents without brain pathology (control subjects), showed the pathological features of mild Alzheimer's disease, with many neocortical plaques. Plaque counts were 80% of those of demented patients with Alzheimer's disease. Choline acetyltransferase and somatostatin levels were intermediate between controls and demented patients with Alzheimer's disease. The unexpected findings in these subjects were higher brain weights and greater number of neurons (greater than 90 micron 2 in a cross-sectional area in cerebral cortex) as compared to age-matched nursing home control subjects. These people may have had incipient Alzheimer's disease but escaped loss of large neurons, or alternatively, started with larger brains and more large neurons and thus might be said to have had a greater reserve.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [9] |
We used path analysis on data from the British 1946 birth cohort to model lifetime antecedents of cognitive reserve, represented by the NART at 53 years, and compared this model for verbal memory and psychomotor function at this age, cognitive outcomes that are sensitive to age-associated decline. We showed independent paths from childhood cognition, educational attainment and adult occupation to cognitive reserve, with that from childhood cognition the strongest, and that from adult occupation the weakest. A similar pattern was found for the verbal memory and psychomotor outcomes, although the pathways were weaker than those to the NART. The pattern was also mirrored by the paths from paternal occupation to childhood cognition, educational attainment and adult occupation, with that to childhood cognition the strongest, and that to adult occupation the weakest. The direct influence of paternal occupation on cognitive reserve was negligible, and almost entirely mediated by childhood cognitive ability and educational attainment.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [10] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [11] |
Few data are available about how social networks reduce the risk of cognitive impairment in old age. We aimed to measure this effect using data from a large, longitudinal, epidemiological clinicopathological study.89 elderly people without known dementia participating in the Rush Memory and Aging Project underwent annual clinical evaluation. Brain autopsy was done at the time of death. Social network data were obtained by structured interview. Cognitive function tests were Z scored and averaged to yield a global and specific measure of cognitive function. Alzheimer's disease pathology was quantified as a global measure based on modified Bielschowsky silver stain. Amyloid load and the density of paired helical filament tau tangles were also quantified with antibody-specific immunostains. We used linear regression to examine the relation of disease pathology scores and social networks to level of cognitive function.Cognitive function was inversely related to all measures of disease pathology, indicating lower function at more severe levels of pathology. Social network size modified the association between pathology and cognitive function (parameter estimate 0.097, SE 0.039, p=0.016, R(2)=0.295). Even at more severe levels of global disease pathology, cognitive function remained higher for participants with larger network sizes. A similar modifying association was observed with tangles (parameter estimate 0.011, SE 0.003, p=0.001, R(2)=0.454). These modifying effects were most pronounced for semantic memory and working memory. Amyloid load did not modify the relation between pathology and network size. The results were unchanged after controlling for cognitive, physical, and social activities, depressive symptoms, or number of chronic diseases.These findings suggest that social networks modify the relation of some measures of Alzheimer's disease pathology to level of cognitive function.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [12] |
Cognitive reserve (CR) shows protective effects in Alzheimer's disease (AD) and reduces the risk of dementia. Despite the clinical significance of CR, a clinically useful diagnostic biomarker of brain changes underlying CR in AD is not available yet. Our aim was to develop a fully-automated approach applied to fMRI to produce a biomarker associated with CR in subjects at increased risk of AD. We computed resting-state global functional connectivity (GFC), i.e. the average connectivity strength, for each voxel within the cognitive control network, which may sustain CR due to its central role in higher cognitive function. In a training sample including 43 mild cognitive impairment (MCI) subjects and 24 healthy controls (HC), we found that MCI subjects with high CR (> median of years of education, CR+) showed increased frequency of high GFC values compared to MCI-CR- and HC. A summary index capturing such a surplus frequency of high GFC was computed (called GFC reserve (GFC-R) index). GFC-R discriminated MCI-CR+ vs. MCI-CR-, with the area under the ROC = 0.84. Cross-validation in an independently recruited test sample of 23 MCI subjects showed that higher levels of the GFC-R index predicted higher years of education and an alternative questionnaire-based proxy of CR, controlled for memory performance, gray matter of the cognitive control network, white matter hyperintensities, age, and gender. In conclusion, the GFC-R index that captures GFC changes within the cognitive control network provides a biomarker candidate of functional brain changes of CR in patients at increased risk of AD.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [13] |
More educated elders are less susceptible to age-related or pathological cognitive changes. We aimed at providing a comprehensive contribution to the neural mechanism underlying this effect thanks to a multimodal approach. Thirty-six healthy elders were selected based on neuropsychological assessments and cerebral amyloid imaging, i.e. as presenting normal cognition and a negative florbetapir-PET scan. All subjects underwent structural MRI, FDG-PET and resting-state functional MRI scans. We assessed the relationships between years of education and i) gray matter volume, ii) gray matter metabolism and iii) functional connectivity in the brain areas showing associations with both volume and metabolism. Higher years of education were related to greater volume in the superior temporal gyrus, insula and anterior cingulate cortex and to greater metabolism in the anterior cingulate cortex. The latter thus showed both volume and metabolism increases with education. Seed connectivity analyses based on this region showed that education was positively related to the functional connectivity between the anterior cingulate cortex and the hippocampus as well as the inferior frontal lobe, posterior cingulate cortex and angular gyrus. Increased connectivity was in turn related with improved cognitive performances. Reinforcement of the connectivity of the anterior cingulate cortex with distant cortical areas of the frontal, temporal and parietal lobes appears as one of the mechanisms underlying education-related reserve in healthy elders. Copyright © 2013 Elsevier Inc. All rights reserved.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [14] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [15] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [16] |
In Alzheimer's disease (AD), the cognitive reserve theory predicts that at any level of assessed clinical severity, the underlying brain pathology is more advanced in patients with more cognitive reserve. Recent evidences suggest that cerebrospinal fluid (CSF) biomarkers may reflect the brain pathology in AD. We investigated the relationship between education level and CSF concentrations of β-amyloid, total tau and phosphorylated tau (ptau-181) in a cohort of 70 subjects newly diagnosed with AD. We report that CSF concentration of β-amyloid was inversely associated with years of education, after adjustment for age, sex, and severity of the disease. We further demonstrate in stratified analysis that this relation was mainly present in mild form of the disease (CDR1), and was attenuated in more advanced forms of the disease. These results are consistent with the cognitive reserve theory, and suggest that cognitive reserve may be protective against amyloid related cognitive impairment at the onset of the clinical dementia.Copyright © 2010 Elsevier Inc. All rights reserved.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [17] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [18] |
靳飞, 刘怀贵, 李伟, 等. 基于静息态功能连接模式的正常人脑扣带皮层亚区划分[J]. 中国医学影像技术, 2016, 32(1): 30-34.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [19] |
The apolipoprotein E (APOE) ε4 allele increases the risk for late-onset Alzheimer's disease (AD) and age-related cognitive decline. We investigated whether ε4 carriers show reductions in gray matter volume compared with ε4 non-carriers decades before the potential onset of AD dementia or healthy cognitive aging. Fourteen cognitively normal ε4 carriers, aged 26 to 45 years, were compared with 10 age-matched, ε4 non-carriers using T1-weighted volumetric magnetic resonance imaging (MRI) scans. All had reported first- or second-degree family histories of dementia. Group differences in gray matter were tested using voxel-based morphometry (VBM) and a multivariate model of regional covariance, the Scaled Subprofile Model (SSM). A combination of the first two SSM MRI gray matter patterns distinguished the APOE ε4 carriers from non-carriers. This combined pattern showed gray matter reductions in bilateral dorsolateral and medial frontal, anterior cingulate, parietal, and lateral temporal cortices with covarying relative increases in cerebellum, occipital, fusiform, and hippocampal regions. With these gray matter differences occurring decades before the potential onset of dementia or cognitive aging, the results suggest longstanding, gene-associated differences in brain morphology that may lead to preferential vulnerability for the later effects of late-onset AD or healthy brain aging.Copyright © 2012 Elsevier Inc. All rights reserved.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| {{custom_ref.label}} |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
PDF(804 KB)
Collection(s)
/
| 〈 |
|
〉 |



{kind=link}
{kind=link}