 PDF(819 KB)
PDF(819 KB)

Correlation between Alzheimer's disease and common chronic diseases
JIANG Yaling, WEN Yafei, LIU Xixi, ZHOU Hui, TANG Beisha, WENG Ling
PDF(819 KB)
Correlation between Alzheimer's disease and common chronic diseases
Objective: To explore the relationship of hypertension, diabetes mellitus and serum lipid levels between AD patients and normal controls. Method: This study included 513 AD patients and 322 normal controls screened by MMSE. Data of hypertension, diabetes, cholesterol, triglyceride, high density lipoprotein and low density lipoprotein were collected. Data of hypertension and diabetes between AD group and control group were analyzed by chi-square test, and serum lipid data was analyzed by t test. Results: The prevalence of hypertension in AD patients was significantly lower than in normal controls, and the difference was statistically significant (P< 0.05); the prevalence of diabetes in AD patients was not significantly correlated with normal controls; the levels of cholesterol, triglycerides and low-density lipoprotein in AD patients were lower than those in normal controls, while high-density lipoprotein levels were higher than that in normal controls, and the differences were statistically significant (P< 0.05). Conclusion: In this study, we found that there are some differences of hypertension and dyslipidemia and no difference of diabetes between AD patients and normal controls. However, based on current results, we are unable to determine whether there is a correlation between AD and hypertension, diabetes and dyslipidemia. Larger sample size and longitudinal researches are needed to determine the relationship.
Alzheimer's disease / Chronic disease / Hypertension / Diabetes mellitus / Dyslipidemia / Comorbidity {{custom_keyword}} /
表1 AD组(513例)、AD血脂组(147例) 和对照组(322例)基本信息表 |
| 项目 | AD组(例) | AD血脂组(例) | 对照组(例) | |
|---|---|---|---|---|
| 性别 | 男 | 189 | 52 | 165 |
| 女 | 324 | 95 | 157 | |
| 年龄段 | 中年(40~64岁) | 195 | 66 | 104 |
| 老年(65~84岁) | 281 | 75 | 208 | |
| 高龄老人(≥85岁) | 37 | 6 | 10 |
表2 不同性别AD组和对照组患高血压情况比较 |
| 性别 | 高血压 | 有(例) | 无(例) | 总计(例) | 卡方值 | P值 |
|---|---|---|---|---|---|---|
| 男性 | AD组 | 51 | 138 | 189 | 9.335 | 0.002* |
| 对照组 | 70 | 95 | 165 | |||
| 总计 | 121 | 233 | 354 | |||
| 女性 | AD组 | 98 | 226 | 324 | 1.778 | 0.182 |
| 对照组 | 57 | 100 | 157 | |||
| 总计 | 155 | 326 | 481 | |||
| 总体 | AD组 | 149 | 364 | 513 | 9.662 | 0.002* |
| 对照组 | 127 | 195 | 322 | |||
| 总计 | 276 | 559 | 835 |
| 注:*示P值< 0.05。 |
表3 不同年龄段AD组和对照组患高血压情况比较 |
| 年龄段 | 高血压 | 有(例) | 无(例) | 总计(例) | 卡方值 | P值 |
|---|---|---|---|---|---|---|
| 中年 | AD组 | 33 | 162 | 195 | 4.958 | 0.026* |
| 对照组 | 29 | 75 | 104 | |||
| 总计 | 62 | 237 | 299 | |||
| 老年 | AD组 | 102 | 179 | 281 | 3.936 | 0.047* |
| 对照组 | 94 | 114 | 208 | |||
| 总计 | 196 | 293 | 489 | |||
| 高龄 老人 | AD组 | 14 | 23 | 37 | 0.000 | 1.000 |
| 对照组 | 4 | 6 | 10 | |||
| 总计 | 18 | 29 | 47 |
| 注:*示P值< 0.05。 |
表4 不同性别AD组和对照组患糖尿病情况比较 |
| 性别 组别 | 糖尿病 | 卡方值 | P值 | |||
|---|---|---|---|---|---|---|
| 有(例) | 无(例) | 总计(例) | ||||
| 男性 | AD组 | 17 | 172 | 189 | 3.776 | 0.072 |
| 对照组 | 26 | 139 | 165 | |||
| 总计 | 43 | 311 | 354 | |||
| 女性 | AD组 | 31 | 293 | 324 | 2.131 | 0.144 |
| 对照组 | 22 | 135 | 157 | |||
| 总计 | 53 | 428 | 481 | |||
| 总体 | AD组 | 48 | 465 | 513 | 5.989 | 0.014* |
| 对照组 | 48 | 274 | 322 | |||
| 总计 | 96 | 739 | 835 | |||
| 注:*示P值< 0.05。 |
表5 不同年龄段AD组和对照组患糖尿病情况比较 |
| 年龄段 组别 | 糖尿病 | 卡方值 | P值 | |||
|---|---|---|---|---|---|---|
| 有(例) | 无(例) | 总计(例) | ||||
| 中年 | AD组 | 11 | 184 | 195 | 0.142 | 0.706 |
| 对照组 | 7 | 97 | 104 | |||
| 总计 | 18 | 281 | 299 | |||
| 老年 | AD组 | 33 | 248 | 281 | 4.673 | 0.031* |
| 对照组 | 39 | 169 | 208 | |||
| 总计 | 72 | 417 | 489 | |||
| 高龄 | AD组 | 4 | 33 | 37 | 0.057 | 0.811 |
| 对照组 | 2 | 8 | 10 | |||
| 总计 | 6 | 41 | 47 | |||
| 注:*示P值< 0.05。 |
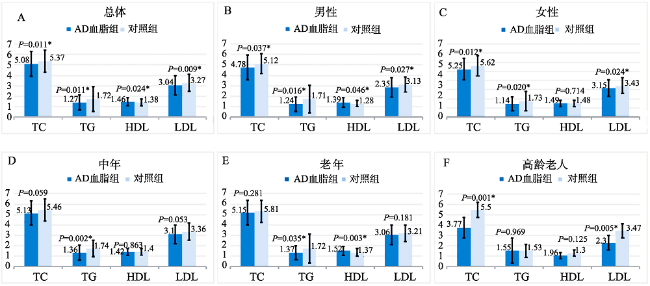
表6 不同性别AD血脂组与对照组的TC、TG、HDL和LDL水平比较(±s, mmol/L) |
| 性别 | 组别 | 人数(例) | TC | TG | HDL | LDL |
|---|---|---|---|---|---|---|
| 男性 | AD血脂组 | 52 | 4.78±1.20 | 1.24±0.69 | 1.39±0.47 | 2.85±0.93 |
| 对照组 | 165 | 5.12±0.94 | 1.71±1.33 | 1.28±0.30 | 3.13±0.74 | |
| P值 | 0.037* | 0.016* | 0.046* | 0.027* | ||
| 女性 | AD血脂组 | 95 | 5.25±1.17 | 1.44±0.72 | 1.49±0.34 | 3.15±0.91 |
| 对照组 | 157 | 5.62±1.10 | 1.73±1.06 | 1.48±0.36 | 3.41±0.87 | |
| P值 | 0.012* | 0.020* | 0.714 | 0.024* | ||
| 总体 | AD血脂组 | 147 | 5.08±1.20 | 1.37±0.72 | 1.46±0.40 | 3.04±0.92 |
| 对照组 | 322 | 5.37±1.05 | 1.72±1.20 | 1.38±0.34 | 3.27±0.82 | |
| P值 | - | 0.011* | 0.001* | 0.024* | 0.009* |
| 注:*示P值< 0.05。 |
表7 不同年龄段AD血脂组与对照组的TC、TG、HDL和LDL水平比较(±s, mmol/L) |
| 年龄段 | 组别 | 人数(例) | TC | TG | HDL | LDL |
|---|---|---|---|---|---|---|
| 中年 | AD血脂组 | 66 | 5.13±1.17 | 1.36±0.73 | 1.42±0.31 | 3.10±0.89 |
| 对照组 | 104 | 5.46±1.07 | 1.74±0.81 | 1.40±0.33 | 3.36±0.84 | |
| P值 | - | 0.059 | 0.002* | 0.653 | 0.053 | |
| 老年 | AD血脂组 | 75 | 5.15±1.19 | 1.37±0.66 | 1.52±0.45 | 3.06±0.95 |
| 对照组 | 208 | 5.31±1.05 | 1.72±1.38 | 1.37±0.35 | 3.21±0.81 | |
| P值 | - | 0.281 | 0.035* | 0.003* | 0.181 | |
| 高龄老人 | AD血脂组 | 6 | 3.77±1.01 | 1.55±1.22 | 1.06±0.30 | 2.30±0.70 |
| 对照组 | 10 | 5.50±0.72 | 1.53±0.61 | 1.30±0.29 | 3.47±0.70 | |
| P值 | - | 0.001* | 0.969 | 0.125 | 0.005* |
| 注:*示P值< 0.05。 |
| [1] |
International Alzheimer’s Disease. World Alzheimer Report 2018[R]. 2019.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [2] |
Querfurth, HW, Laferla, FM. Alzheimer’s disease[J]. N Engl J Med, 2010, 362(4): 329-344.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [3] |
张振馨, 洪霞, 李辉, 等. 北京城乡55岁或以上居民简易智能状态检查测试结果的分布特征[J]. 中华神经科杂志, 1999(3): 20-24.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [4] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [5] |
世界卫生组织. 全球糖尿病报告[R].
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [6] |
周建红, 陈建强. 6048名社区老年人体检情况分析[J]. 检验医学与临床, 2017, 14(3): 415-417.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [7] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [8] |
To test the hypothesis that hypertension, high blood pressure, and high pulse pressure (PP) are independently associated with lower cognitive function.Cross-sectional study of persons examined in 1988 to 1994.U.S. noninstitutionalized population.Six thousand one hundred sixty-three men and women aged 60 and older who participated in the Third National Health and Nutrition Examination Survey (NHANES III).Measurements included blood pressure, short-portable Mini-Mental State Examination (sp-MMSE), self-reported history of hypertension, diagnosis, and treatment.In the initial bivariate analysis within age groups of 60 to 64, 65 to 69, and 70 to 74, optimal blood pressure (< 120/80 mmHg) was associated with best cognitive performance; the severe hypertension group had the poorest performance in all age groups except the very old (> or = 80), where the pattern was reversed, showing poorest performance in the optimal blood pressure group and best in the group with moderate hypertension. This pattern changed slightly in multiple regression analyses modeling sp-MMSE as the outcome variable. Higher stage of hypertension according to the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure and higher PP were associated with worse cognitive performance than normal blood pressure at ages 70 to 79 and 80 and older. No significant negative association was seen in subjects aged 60 to 69. Subjects with treated but uncontrolled hypertension had significantly lower sp-MMSE scores than those without hypertension or with controlled hypertension after controlling for age, sex, ethnicity, income, and PP.At age 70 and older, high blood pressure, hypertension, and uncontrolled blood pressure are associated with poorer cognitive function than normal blood pressure. Optimal control of blood pressure may be useful in preserving neurocognitive loss as the population ages.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [9] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [10] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [11] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [12] |
Autonomic dysfunction is very common in patients with dementia, and its presence might also help in differential diagnosis among dementia subtypes. Various central nervous system structures affected in Alzheimer's disease are also implicated in autonomic nervous system regulation, and it has been hypothesized that the deficit in central cholinergic function observed in Alzheimer's disease could likely lead to autonomic dysfunction. Several feasible tests can be used in clinical practice for the assessment of parasympathetic and sympathetic functions, especially in terms of cardiovascular autonomic modulation. In this review, we describe the different tests available and the evidence from the literature which indicate a definite presence of autonomic dysfunction in dementia at various degrees. Importantly, the recognition of dysautonomia, besides possibly being an early marker of dementia, would help prevent the disabling complications which increase the risk of morbidity, institutionalization, and mortality in these individuals.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [13] |
Autonomic function has received little attention in Alzheimer's disease (AD). AD pathology has an impact on brain regions which are important for central autonomic control, but it is unclear if AD is associated with disturbance of autonomic function.To investigate autonomic function using standardized techniques in patients with AD and healthy age-matched controls.Thirty-three patients with mild to moderate AD and 30 age- and gender-matched healthy controls, without symptoms of autonomic dysfunction, underwent standardized autonomic testing with deep breathing, Valsalva maneuver, head-up tilt, and isometric handgrip test. Brachial pressure curve and electrocardiogram were recorded for off-line analysis of blood pressure and beat-to-beat heart rate (HR).AD patients had impaired blood pressure responses to Vasalva maneuver (p < 0.0001) and HR response to isometric contraction (p = 0.0001). A modified composite autonomic scoring scale showed greater degree of autonomic impairment in patients compared to controls (patient: 2.1 ± 1.6; controls: 0.9 ± 1.1, p = 0.001). HR response to deep breathing and Valsalva ratio were similar in the two groups.We identified autonomic impairment ranging from mild to severe in patients with mild to moderate AD, who did not report autonomic symptoms. Autonomic impairment was mainly related to impairment of sympathetic function and evident by impaired blood pressure response to the Vasalva maneuver. The clinical implications of this finding are that AD may be associated with autonomic disturbances, but patients with AD may rarely report symptoms of autonomic dysfunction. Future research should systematically evaluate symptoms of autonomic function and characterize risk factors associated with autonomic dysfunction.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [14] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [15] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [16] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [17] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [18] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [19] |
Historically, insulin is best known for its role in peripheral glucose homeostasis, and insulin signaling in the brain has received less attention. Insulin-independent brain glucose uptake has been the main reason for considering the brain as an insulin-insensitive organ. However, recent findings showing a high concentration of insulin in brain extracts, and expression of insulin receptors (IRs) in central nervous system tissues have gathered considerable attention over the sources, localization, and functions of insulin in the brain. This review summarizes the current status of knowledge of the peripheral and central sources of insulin in the brain, site-specific expression of IRs, and also neurophysiological functions of insulin including the regulation of food intake, weight control, reproduction, and cognition and memory formation. This review also considers the neuromodulatory and neurotrophic effects of insulin, resulting in proliferation, differentiation, and neurite outgrowth, introducing insulin as an attractive tool for neuroprotection against apoptosis, oxidative stress, beta amyloid toxicity, and brain ischemia.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [20] |
Arduous efforts have been made in the last three decades to elucidate the role of insulin in the brain. A growing number of evidences show that insulin is involved in several physiological function of the brain such as food intake and weight control, reproduction, learning and memory, neuromodulation and neuroprotection. In addition, it is now clear that insulin and insulin disturbances particularly diabetes mellitus may contribute or in some cases play the main role in development and progression of neurodegenerative and neuropsychiatric disorders. Focusing on the molecular mechanisms, this review summarizes the recent findings on the involvement of insulin dysfunction in neurological disorders like Alzheimer's disease, Parkinson's disease and Huntington's disease and also mental disorders like depression and psychosis sharing features of neuroinflammation and neurodegeneration.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [21] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [22] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [23] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [24] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [25] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [26] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [27] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [28] |
Amyloid beta (Aβ), the hallmark of Alzheimer's Disease (AD), now appears to be deleterious in its low number aggregate form as opposed to the macroscopic Aβ fibers historically seen postmortem. While Alzheimer targets, such as the tau protein, amyloid precursor protein (APP) processing, and immune system activation continue to be investigated, the recent discovery that amyloid beta aggregates at lipid rafts and likely forms neurotoxic pores has led to a new paradigm regarding why past therapeutics may have failed and how to design the next round of compounds for clinical trials. An atomic resolution understanding of Aβ aggregates, which appear to exist in multiple conformations, is most desirable for future therapeutic development. The investigative difficulties, structures of these small Aβ aggregates, and current therapeutics are summarized in this review.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [29] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [30] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [31] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [32] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [33] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| {{custom_ref.label}} |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
PDF(819 KB)
 表1 AD组(513例)、AD血脂组(147例) 和对照组(322例)基本信息表表2 不同性别AD组和对照组患高血压情况比较表3 不同年龄段AD组和对照组患高血压情况比较表4 不同性别AD组和对照组患糖尿病情况比较表5 不同年龄段AD组和对照组患糖尿病情况比较表6 不同性别AD血脂组与对照组的TC、TG、HDL和LDL水平比较(±s, mmol/L)
表1 AD组(513例)、AD血脂组(147例) 和对照组(322例)基本信息表表2 不同性别AD组和对照组患高血压情况比较表3 不同年龄段AD组和对照组患高血压情况比较表4 不同性别AD组和对照组患糖尿病情况比较表5 不同年龄段AD组和对照组患糖尿病情况比较表6 不同性别AD血脂组与对照组的TC、TG、HDL和LDL水平比较(±s, mmol/L) 图1 AD血脂组与对照组的TC、TG、HDL和LDL水平比较表7 不同年龄段AD血脂组与对照组的TC、TG、HDL和LDL水平比较(±s, mmol/L)
图1 AD血脂组与对照组的TC、TG、HDL和LDL水平比较表7 不同年龄段AD血脂组与对照组的TC、TG、HDL和LDL水平比较(±s, mmol/L)/
| 〈 |
|
〉 |

{kind=link}